UNFPA works to comprehensively address gender-based violence across the continuum of humanitarian, development and peace-responsive actions in more than 150 countries and territories around the world. In 2022 alone, UNFPA invested more than $454 million in eliminating gender-based violence and harmful practices.
UNFPA works in partnership with women’s and youth feminist organizations, networks and movements; civil-society organizations; governments; academic and research institutes; and other partners to support initiatives to end violence against women, including through prevention programming, service delivery, policy and laws, and data and research.
Responding to gender-based violence in all contexts
UNFPA supports comprehensive, survivor-centred responses in humanitarian and development settings through quality health care, social services, and legal and justice support. At the core of UNFPA’s approach are the rights to safety, confidentiality, non-discrimination and self-determination for all survivors. Guidance is available in the Flourish: UNFPA Gender-based Violence Operational Plan.
To be sure, demographic shifts and challenges linked to climate change, the protracted nature of crises and the frequency of conflicts, as well as population movements, are rendering conventional distinctions between “humanitarian” and “development” programming increasingly irrelevant. In both situations, there is a dramatic increase in gender-based violence. Working across the continuum to respond helps ensure coherence across development, humanitarian and peace-responsive actions. In every context, our initiatives are geared towards strengthening preparedness and promoting long-term development, as well as enhancing local capacities with a focus on risk reduction and resilience building, among others. Key guidance documents: UNFPA Strategy and Operational Plan to Scale Up and Strengthen Interventions on Gender-Based Violence in Emergencies 2023–2025 and Addressing Gender-Based Violence Across Contexts.
One key initiative for survivors is the integration of essential services on sexual and reproductive health into programmes, policies and advocacy across many sectors. As health services are among the first places that survivors seek assistance, UNFPA leverages this opportunity to reach affected women and girls. Those in need of support may be linked to case-management services and referred to support such as life-saving medical services and supplies, cash or voucher assistance, dignity kits containing essential items, and psychosocial services and legal support.
From 2023 to 2026, UNFPA is implementing Women at the Centre, a global programme that seeks to improve the accessibility and availability of quality response services for survivors of gender-based violence, with a focus on the most marginalized. The programme is building a professional social-service workforce equipped with the skills needed to strengthen case management in Azerbaijan, El Salvador, Indonesia, Madagascar and Zimbabwe.
Between 2024 and 2027, UNFPA is rolling out Making All Spaces Safe, a global programme tackling the rising and evolving threat of technology-facilitated gender-based violence (TFGBV) globally and nationally in Kenya and Benin. This initiative is bridging existing gaps in addressing TFGBV through comprehensive and survivor-centred programming that integrates digital literacy into prevention and response mechanisms, and mitigates harm through rights-based law reform and safety-by-design standards.
UNFPA also plays a role in setting standards for survivor-centred care in line with the Essential Services Package for Women and Girls Subject to Violence and the Interagency Minimum Standards on Gender-Based Violence in Emergencies Programming. UNFPA is the Inter-Agency Standing Committee–mandated lead agency on gender-based violence in emergencies, leading the Gender-Based Violence Area of Responsibility, the global forum for coordination on prevention, risk mitigation and response in humanitarian settings.
Preventing gender-based violence
The prevalence of gender-based violence is symptomatic of pervasive inequality due to harmful social and gender norms that restrict women and girls from having agency over their own bodies and from participating in economies and decision-making spaces.
In its efforts to end gender-based violence, UNFPA works to change harmful social and gender norms that perpetuate gender inequality. UNFPA works in partnership with UN Women, the World Health Organization and the UN Development Programme to implement strategies to prevent gender-based violence as outlined in the RESPECT framework. For example, UNFPA works with men and boys to promote positive masculinities with the aim of advancing gender equality and ending violence and harmful practices against women and girls, while remaining accountable to feminist movements.
UNFPA also uses comprehensive sexuality education in and out of school as a primary prevention strategy to end gender-based violence, since it helps adolescents nurture positive gender-equitable attitudes and values, which are linked to reduced violence and healthier, equitable, non-violent relationships. This early intervention can have long-lasting impacts across the lives of women and men.
Supporting laws and policies
Gender-based violence is a human rights violation and is the result of structural, deep-rooted discrimination, which requires legislative, administrative and institutional measures and reforms, including the eradication of gender stereotypes.
UNFPA supports governments in the implementation of international agreements including the International Conference on Population and Development, the Sustainable Development Goals, the 2030 Agenda, the Convention on the Elimination of All Forms of Discrimination Against Women and the Beijing Platform for Action. UNFPA has contributed to strengthening national policies and accountability and legal frameworks, including laws on gender-based violence.
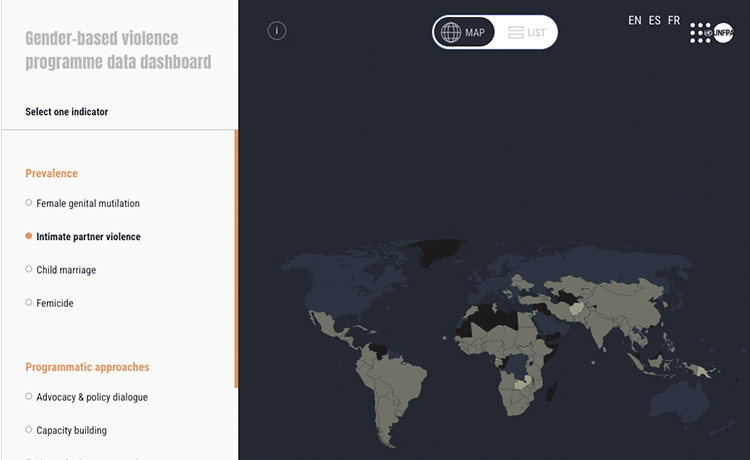
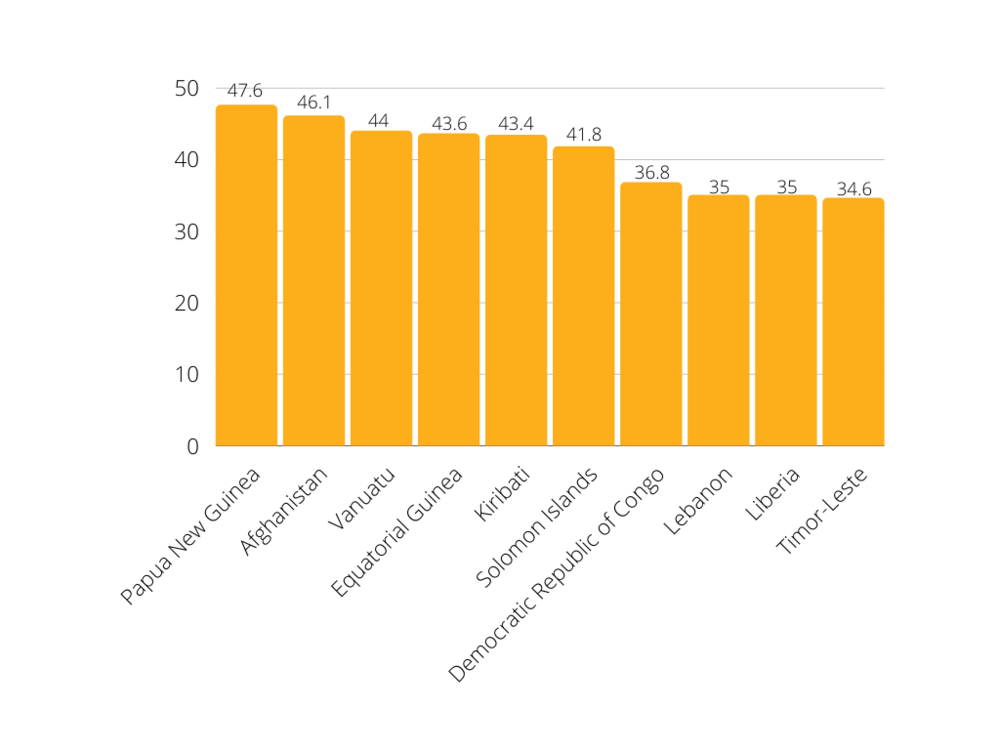
Measuring the problem
UNFPA works extensively in collecting data and generating evidence to understand the prevalence, incidence and impact of gender-based violence worldwide. This provides the foundation for informed decision-making, resource allocation and the development of policies and programmes that have a meaningful impact on reducing gender-based violence.
In 2016, UNFPA and the Australian Department of Foreign Affairs and Trade launched the kNOwVAWdata initiative in the Asia Pacific region. With support from the Joint EU–UN Spotlight Initiative, UNFPA has now scaled up the kNOwVAWdata initiative into a further five regions. This initiative provides quality technical support and capacity building for the ethical collection of evidence, as well as support in translating these data into evidence-based policies.
UNFPA also supports the Gender-Based Violence Information Management System, which is used in crisis settings, as well as an adapted version of this system for development settings. These systems enable the safe collection, storage, analysis and sharing of data reported by survivors.
UNFPA is also a partner in the UN Trust Fund to End Violence Against Women, a global grant-making mechanism that invests in initiatives by civil-society organizations around the world aimed at ending gender-based violence through prevention, law and policy implementation and providing access to essential services for survivors.
Across every nation and cultural context, there is a pressing need for increased activism to guarantee that women and girls, in all their diversity, can lead lives free from violence and coercion. UNFPA actively promotes and supports the prevention and elimination of violence against women and girls in all its forms, including active participation in the 16 Days of Activism against Gender-Based Violence.
Updated 25 November 2024


: Action on Human Rights Recommendations to Advance Gender Equality and Sexual and Reproductive Health and Rights")







